

Tuberculosis has been killing people for thousands of years across the globe. In India Acharya Charak mentions it as Yakshma or Rajayakshma, Hippocrates has also written about it. Even today in 2026, it remains the world’s deadliest infectious disease caused by a single pathogen, responsible for 1.23 million deaths in 2024 according to the WHO. India shoulders the heaviest burden of 25 per cent of all global TB cases and an even 32 per cent of drug-resistant TB.
A study published recently in the international journal Nucleic Acids Research about TB has changed the thinking. A team from Bose Institute, Kolkata an autonomous institute under the Department of Science and Technology has found that a foundational concept in molecular biology, one that has been taught in textbooks for decades does not hold true for Mycobacterium tuberculosis, the bacterium responsible for TB. If they translate these findings into drug development, it could reshape how we fight a disease that has outlasted most of human civilisation.
The rule that wasn’t universal
To understand what the Bose Institute team found, we need a rough sketch of how bacteria run their internal machinery. When a bacterial cell needs to produce a protein, firstly it has to read the instructions encoded in its DNA. That reading process is called transcription and the machine that does it is an enzyme called RNA polymerase. This enzyme is a bit like a car engine with no steering. It needs a navigator. That navigator is a protein called a sigma (σ) factor, which binds to the RNA polymerase and tells it exactly where on the DNA to start transcribing.
For decades, the accepted wisdom was that once transcription gets going, the sigma factor detaches and goes off to initiate another round elsewhere. This orderly handover process was called the sigma-cycle, and it was considered universal across all bacteria. Neat, logical and apparently settled. Team of Dr Jayanta Mukhopadhyay and Dr N. Hazra of Bose Institute have now shown it isn’t happening.
What the Indian scientists actually discovered
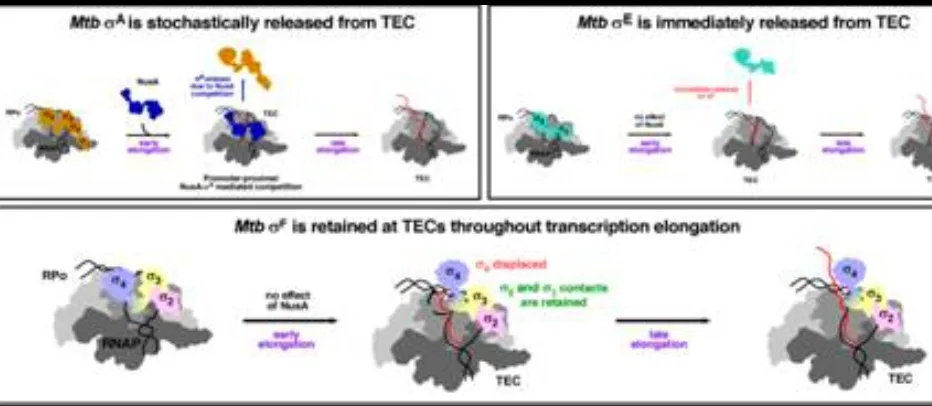
The researchers studied three specific sigma factors in Mycobacterium tuberculosis named σA, σE and σF each has different job. σA handles the bacterium basic, simply housekeeping. σE kicks in under stress conditions, when the environment turns hostile. σF is associated with survival and adaptation in extreme stress, including the kinds of conditions the bacterium encounters inside a human lung.
Using a combination of in vitro transcription assays, fluorescence-based measurements, high resolution protein interaction studies and in vivo validation through chromatin immunoprecipitation and quantitative PCR a formidable experimental toolkit. Then the team tracked how each sigma factor behaved once transcription elongation began. The results were not what the textbook predicted.
σA and σE did detach from RNA polymerase during elongation one immediately, one gradually and broadly following the established sigma-cycle model. σF did nothing of the sort. It stayed firmly attached to the RNA polymerase throughout the entire transcription process. It did not let go. This is not a minor variation on a known theme. It is a categorically different mechanism, one that has not been described before in any bacterium in quite this way.
Why it matters, especially for drug-resistant TB
After rigrous experimentations, it was found that σF’s stubborn attachment to RNA polymerase appears to be the bacterium’s way of ensuring that stress-response genes keep firing, continuously for as long as the stress persists. Inside a human body surrounded by immune cells, starved of nutrients, bathed in hostile chemistry M. tuberculosis is under constant stress. σF now appears as part of how it survives that stress so effectively.
This matters enormously for the drug resistance problem. The standard approach to antibiotic development has long been to target the active sites of bacterial enzymes, the places where the enzyme actually does its chemistry. The problem is that bacteria mutate. And when an active site mutates to avoid a drug, resistance emerges. Broadly speaking why drug-resistant and multidrug-resistant TB strains exist today, why only about two in five people with drug-resistant TB actually access adequate treatment globally and why MDR-TB still claimed an estimated 150,000 lives in 2023.
What the Bose Institute finding points toward is a different kind of target, entirely the protein-protein interaction between σF and RNA polymerase itself. Disrupting this specific molecular handshake the precise interface where σF grips the enzyme could potentially shut down the sustained stress-response transcription that allows the bacterium to persist inside a human host. This interaction is structurally distinct from the enzyme active site. A drug designed to disrupt it would not be easily evaded by the same resistance mutations that have rendered so many existing antibiotics less effective.
India’s burden, Indian science resolving it
India carries a quarter of the world’s TB burden. It has the highest number of MDR-TB cases globally. The WHO’s 2025 Global Tuberculosis Report, released just months ago noted that India diagnosed its highest-ever 26.18 lakh TB cases in 2024 and still has an estimated one lakh cases undetected and silently spreading. The disease is not a distant global health statistic for India. It is present in the country’s cities and villages.
The work of Dr Mukhopadhyay and Dr Hazra and their publication in Nucleic Acids Research, one of the most respected journals in molecular biology places Indian science at the frontier of a field where new ideas are desperately needed. Treatment regimens for drug-resistant TB have been shortened in recent years and India’s treatment success rate under the Pradhan Mantri TB Mukt Bharat Abhiyan is now 90%. But success in detection and treatment of existing strains is a different challenge from defeating the strains that current drugs can’t touch.
Basic science research rarely announces itself with immediate clinical applications. The distance between a molecular discovery and a drug that reaches a patient is long, expensive and uncertain. But it has to start somewhere with someone looking at a bacterium under rigorous experimental conditions and noticing that what the textbook said is not happening. That is precisely what Dr Mukhopadhyay and Dr Hazra did. In a disease as old, as stubborn and as lethal as tuberculosis, the next breakthrough almost certainly begins not in a clinical trial, but in a laboratory in Kolkata asking whether we’ve been reading the biology right all along.















