For more than four decades, encephalitis had threatened the lives of eastern Uttar Pradesh. Every monsoon, districts such as Gorakhpur, Kushinagar, Maharajganj, Deoria, Basti, and Siddharthnagar prepare themselves not only for floods but for an invisible epidemic that follows from stagnant water. Official data between 2010 to 2013 records that encephalitis was not an episodic outbreak but a structural public health failure.
In these four decades, more than one lakh children lost their lives, while several lakhs survived with permanent physical or cognitive disabilities. The disease remained confined to the margins of policy discourse, treated as a seasonal medical challenge rather than a long-term governance issue, with broken sanitation systems and fragile healthcare. Children were its primary victims. High fever, convulsions and sudden neurological collapse became a recurring pattern for the families across villages.
Even before the delivery of governance outcomes, the present Chief Minister of Uttar Pradesh, Yogi Adityanath, has been a voice for eastern Uttar Pradesh as the encephalitis toll continued to claim thousands of young lives. His constant presence in Parliament as a member and in protests has ensured that a regional tragedy became a state mission. In 2025 zero encephalitis death was in Uttar Pradesh.
When healthcare infrastructure failed the region
The persistence of encephalitis was closely linked to the condition of the public health infrastructure in rural eastern Uttar Pradesh. Primary Health Centres and Community Health Centres were chronically understaffed before 2017. Doctors posted under national schemes were often absent at night, referral systems were weak and early-stage treatment was rarely available at the village level. As a result, critically ill children were referred to Lucknow or Varanasi over long distances, often loses life due to reaching hospitals too late.
Baba Raghav Das (BRD) Medical College in Gorakhpur emerged as the region’s final refuge for those who cannot travel to large distances. The documents describe how this single institution carried the burden of patients from dozens of districts, leading to overcrowded wards and intense pressure during peak monsoon months. Administrative neglect meant that even when resources were sanctioned, utilisation remained uneven, reinforcing a cycle in which preventable deaths continued year after year.
From Parliament to public protest
Yogi Adityanath, Member of Parliament from Gorakhpur in 2003, became associated with the encephalitis issue. The documented news source confirms that his engagement began through parliamentary interventions and formal representations to district and state authorities. However, responses remained limited to assurances, and the strategy shifted from institutional advocacy to public mobilisation.
From 2010 onwards, encephalitis became a central issue in sustained protests. The movement records describe sit-ins at district headquarters, mass demonstrations and memoranda addressed to senior administrative officials and the President of India. The emphasis throughout was on accountability, arguing that repeated child deaths reflected systemic failure rather than medical inevitability.
A movement that refused to disperse
Between 2010 and 2013, the encephalitis agitation took the form of a continuous, multi-phase movement rather than isolated protests. In 2011, a four-stage programme unfolded over several weeks, involving dharnas, padyatras from BRD Medical College to the Commissioner’s office, torch marches, signature campaigns and village-level awareness drives. These actions drew participation from social organisations, local residents and families directly affected by the disease.
The demands articulated during these protests remained consistent for declaration of encephalitis as a national epidemic, a dedicated national eradication programme, assured funding, strengthening of district-level healthcare, clean drinking water, sanitation, vector control and rehabilitation for disabled children. The documents underline that encephalitis was framed not merely as a medical issue but as an outcome of rural neglect and uneven development.
Defending treatment capacity and expanding the lens
A major defining episode occurred in October 2011, when proposals of the Samajwadi Party emerged that would have diluted or shifted encephalitis treatment facilities away from BRD Medical College. The response was immediate. A satyagraha inside the medical college campus forced the withdrawal of the proposal, preserving BRD’s role as the region’s primary treatment centre.
At the same time movement broadened its focus. Encephalitis was increasingly linked to unsafe drinking water, poor sanitation, stagnant drains, pig-rearing near human settlements and the absence of sustained vaccination drives. This shift was significant, as it was anticipated in later policy with recognition that Acute Encephalitis Syndrome was not only mosquito-borne but also deeply connected to water contamination and hygiene failures
Data that reflected a slow decline before 2017
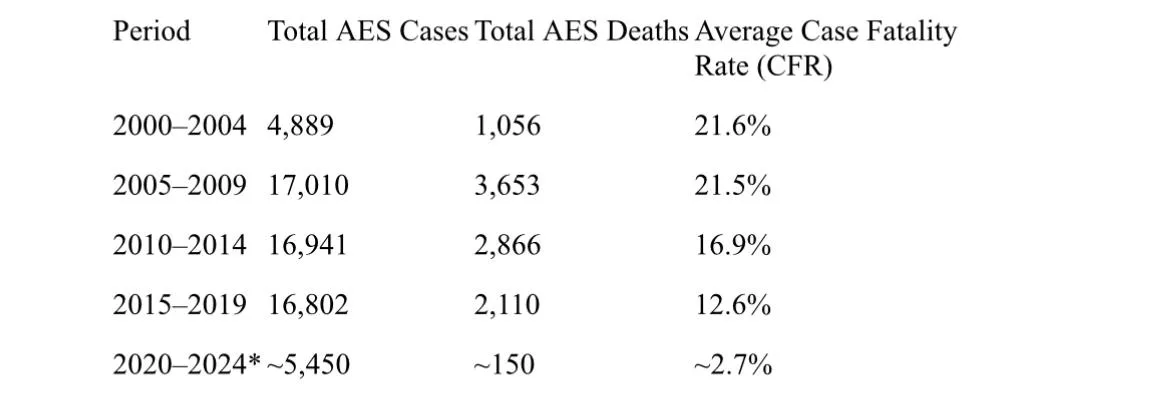
Official data over the years have shown gradual but insufficient improvement before 2017. According to compiled government figures, AES cases and deaths remained high through the early 2000s and the following decade. Between 2000 and 2004, there were 4,889 AES cases with 1,056 deaths, reflecting a case fatality rate of over 21%. The situation worsened between 2005 and 2009, when cases rose to 17,010 and deaths to 3,653.
Although some decline was visible between 2010 and 2014, with deaths reducing to 2,866, the overall burden remained substantial. The period from 2015 to 2019 still recorded over 16,800 cases and more than 2,100 deaths, underscoring that incremental measures were insufficient to dismantle the disease’s structural drivers
UP Encephalitis Data: 5-yearly comparisons (2000–2024)
 2024 data reflects the zero death milestone reported as of late 2024
2024 data reflects the zero death milestone reported as of late 2024
From protest demands to policy after 2017
A decisive shift occurred after March 2017, when Yogi Adityanath assumed office as Chief Minister of Uttar Pradesh. The continuity between earlier movement demands and subsequent policy action was evident. Encephalitis control was taken up in mission mode, with coordinated involvement of health, rural development, drinking water, sanitation, urban development and women-child welfare departments.
Medical infrastructure was strengthened across endemic districts. BRD Medical College and district hospitals saw expansion of paediatric ICU facilities, better oxygen management and improved referral systems. Japanese Encephalitis vaccination coverage was scaled up under the Universal Immunisation Programme, while fogging and vector control were institutionalised as routine preventive measures rather than seasonal reactions.
The integration of clean water and sanitation initiatives started taking place. Under the Swachh Bharat Mission and Jal Jeevan Mission, rural households in eastern Uttar Pradesh received toilets and piped drinking water connections, addressing the water-borne dimensions of AES that the movement had long highlighted.
Measurable outcomes and a broader lesson
The impact of these combined interventions became visible in official data after 2020. Between 2020 and 2024, AES cases dropped to approximately 5,450, with deaths reducing to around 150. The average case fatality rate fell sharply to below 3 per cent. Japanese Encephalitis deaths declined to near zero in several districts, and Gorakhpur gradually shed its long-standing association with encephalitis mortality
The encephalitis death story of eastern Uttar Pradesh thus illustrates a broader governance lesson. For decades, the causes of the crisis were known, but fragmented implementation allowed it to persist. The movement documented from 2010 to 2013 stands as a record of public resistance against institutional inertia. The post-2017 phase demonstrates how sustained political ownership, administrative coordination, and infrastructure-led public health interventions can reverse even deeply entrenched epidemics.
Closing a long chapter of preventable loss
Encephalitis was once regarded as an unavoidable feature of life in eastern Uttar Pradesh. The records of protest, policy neglect and gradual reform show otherwise. What changed was not the nature of the disease, but the seriousness with which governance addressed its causes. While rehabilitation of survivors and long-term surveillance remain ongoing responsibilities. The steep decline in deaths marks one of India’s most consequential public health turnarounds achieved through continuity between public mobilisation and state action rather than abrupt or symbolic intervention.