

Dr Abhay Jere
India is home to the third largest HIV/AIDS affected people in the world with an estimated population of 2.4 million. In the year 2003, sensing the urgency to the curb spread of HIV infection, the Bill and Melinda Gates Foundation (BMGF) designed one of the largest and most promising HIV prevention programmes in the world “Avahan” (“a call to action” in Sanskrit). Avahan was rolled out in six Indian states (Andra Pradesh, Maharashtra, Karnataka, Tamil Nadu, Nagaland and Manipur) as well as key trucking routes, covering approximately 83 per cent of the total HIV population in the country.
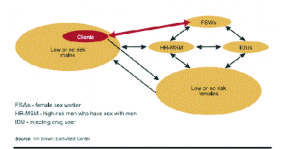
Data from published studies and sentinel surveillance of high-risk groups in India (in 2003) indicated that two factors primarily contribute to the growth of the HIV epidemic i.e., the sex workers and their clients, and the frequency of unprotected sex between them.Men who have sex with men (MOM)and intravenous drug users are also at risk and contribute to the overall epidemic. Moreover, studies showed that HIV transmission in South India was primarily through sexual route, while in the North-East it was mainly related to injecting drug usage.
Although, India’s national response for HIV/AIDS prevention through National AIDS Control Organisation’s (NACO) and National AIDS Control Programme (NACP-I&II) had a comprehensive strategy, its penetration and coverage within the high risk groups was variable and in general low. Hence, the BMGF through programme ‘Avahan’ decided to comprehensively target high risk groups and bridge the population by raising preventive coverage amongst these groups.This will eventually help restrict the transmission of HIV to the general population.
Avahan is a ten years two phase programme and for that BMGF initially committed $258 million which was later increased to $338 million in the year 2009. Also the same year, an MOU was signed between Indian government and the BMGF allowing transfer of Avahan to the Indian government in phases till 2014.As per the MOU, Avahan will be fully owned by Indian government after 2014.
Recently, BMGF announced that it has started winding up its involvement in Avahan and they will only fund the project only till June 2013 while after that they will continue to give only technical support to the government till 2014.Moreover, BMGF’s India head Ashok Alexander who had spearheaded Avahan has also decided to step down.
So after spending $338 million and nine years, what Avahan achieved?
Avahan was initiated with three primary goals:
1. Build an HIV prevention model at large scale in India.
2. Catalyse others to take over and replicate the model.
3. Foster and disseminate learnings within India and worldwide.
To achieve these goals, strategy adopted in Avahan was on prevention efforts within high risk groups using global best practices in HIV prevention, scaling up services rapidly across geographies and investing in knowledge building, evaluation and dissemination. For preventive efforts, Avahan focused on education, giving clinical services to treat Sexually Transmitted Infections (STIs) and aggressively promoting and distributing free condoms for sex workers and needles and syringes to the intravenous drug users. It also focused on facilitating community mobilisation and promoting community ownership of the programme.
Whether Avahan delivered on all or any of the three primary goals?
On analysing the fact sheets released by BMGF and other published reports (currently available data is only till 2009 and BMGF is currently analysing the data post 2009), it can be said with certainty that Avahan emerged as a large scale HIV intervention programme which operated in six high prevalence states with combined population of 300 million. As per the reports, Avahan operated in 605 towns and provided intervention services to more than 220,000 female sex workers, 80,000 high risk MOM, 18,000 injection drug users and five million men at risk along the nation’s major trucking route. The report also claims to establish 800 clinics and provided free STI diagnosis and treatment services for an estimated 340,000 individuals. However, the biggest success which is often highlighted for Avahan is the scale up in condom promotion and distribution programme. Avahan helped scale condom distribution which went up to ten million per month in 2009 (as compared to one million in 2004) to sex workers, high risk MOM and injection drug users. Due to their multidimensional coherent efforts, BMGF claims in the report published in Lancet that Avahan help averted more than 100,000 new infections at the population level between years 2003-2008.
Although, Avahan is successful in building a large scale model (goal-1), the programme has been widely criticised for its extravaganza in terms of expenditure and its faulty implementation.Also, initiallyAvahan had no concrete implementation strategy neither there was any roadmap for BMGF’s exit and handing the project to the government in a systematic fashion.
Avahan started with a bang in six states, with 50 sites for truckers in the south. But by mid-2005, only 12 per cent of truck drivers were even aware of their services, and only 7 per cent took advantage of them. This forced Avahan to reduce the sites to 20. For similar reasons, Avahan”s 6,000 Sexually Transmitted Infection (STI) centres were brought down to just 800. Internal analysis also showed that peer educators were not as effective as they were expected to perform.
If insiders in NACO or health ministry are to be believed, they find Avahan very difficult to sustain considering its high salary structure and the management cost. Also, a large chunk of the budget was spent on expensive travels and extravagant meetings. The cost incurred on management, infrastructure and administrative related expenses was as high as 40 per cent in Avahan as compared to 10 per cent in the government setting although the basic implementation cost per most-at-risk population was more or less the same. Because of this associated high cost, NACO and Health Ministry officials are now not very keen on taking over the programme. Officials believe that if Indian government has to run Avahan successfully in future, costs need to be brought down but they can”t figure out how. They also fears Avahan”s now-experienced MBA-graduates, facing shrinking salaries, will depart and the question of running air-conditioned clinics like Avahan simply doesn”t even arise.
Investment of $338 million went into Avahan for covering just six states, further scaling it up to make it pan-India programme will be extremely resource intensive, thus putting a question mark on its scalability and its chances of replication or adopt as a model in other diseases settings. (Goal 1 &2 not fully achieved).
Another major problem which got highlighted was that of the education material. The material used for creating awareness amongst illiterate or semi-literate sex workers was mostly printed in English which sex workers could hardly read.
The biggest success highlighted of Avahan is the scale achieved in condom promotion, distribution and usage; however the cost incurred is quite disproportionate to the numbers achieved. Moreover, NACO was also simultaneously implementing its NACP-II which would have also contributed to this success.
Regarding the goal 3, which is fostering and dissemination of learning from the study; BMGF is presently understanding and analysing the complete data, based on which critical outcomes and learning might get published in near future.
Although achievements of Avahan cannot be discounted, it did falter in many instances. It success especially in the State of Maharashtra was very poor. But still there are lot of learning which NACO/ Health Ministry can take from Avahan, especially its strategic approach towards building a large scale model and its implementation through a solid network of partnering NGOs. Avahan is also systematically institution-alising the knowledge gained.
Post 2014, to sustain Avahan, Indian government might have to bring down or rationalise the operational cost or even might have to reorient the programme but Avahan must be allowed to sustain as our fight against HIV is still far from over.
(Source: Em Brown, East West Centre)
(The writer can be contacted at [email protected]).









